What are the types of Cataracts?
- Cataracts are basically of three types:
- Congenital or Developmental Cataracts
- Acquired Cataracts
- Senile (age related) Cataracts
What are Congenital or Developmental Cataracts?
Cataracts can develop at any age. New-borns can have cataracts due to infection in the womb commonly due to Rubella, metabolic imbalances, and infections.
Any blow to the eye in play and even severe malnutrition can lead to cataract in childhood.
What are Acquired Cataracts?
These are cataracts occurring in an adult or child following injury to the eye (blunt or penetrating), or sometimes following inflammation in the eye. They can also be caused by excessive exposure to infra-red radiation, (glass blowers cataract seen in people who work with molten glass and steel mill workers) X-rays, ultrasonic, nuclear or microwave radiation.
Our farmers who work long hours in the sun get a cataract sometimes by age 40 which city folk won’t have. Also, our fisherfolk who spend days at sea suffer from early acquired cataract as the UV light from the sun bounces off the water and goes straight into the eye.
Various diseases in the body can be associated with or ‘complicated’ by the presence of a cataract. These are then termed as “Complicated Cataracts”. Typical examples of complicated cataracts are those occurring in diabetes, parathyroid deficiency and following some skin disorders like scleroderma. (However, what this term does not mean is that the cataract has become complicated or sick, or that the surgery is complicated, which is not really the case at all). Eye diseases like “uveitis” can also cause a cataract.
If a cataract arises because of diabetes, parathyroid problems or along with diseases like Lupus SLE etc. the cataract is termed “complicated”. This does not mean the cataract is difficult to remove, nothing like that at all. Inflammation in the eye or even a retinal detachment can lead to cataract. These too are termed,” complicated”. Glaucoma and even retinal detachment can give rise to, “complicated cataract”.
Unlike Europe most of India doesn’t see snow. In Europe people who ski a lot also have UV light bouncing into the eye and causing cataracts and “snow blindness”. This is why you see professional skiers on a seemingly cloudy day wearing really dark sunglasses. All of us, lovers of the outdoors and sailors as well must protect ourselves from the sun with UV protecting glasses.
Does a “complicated cataract” need special management?
Not really. The latest tools like Robotic total laser cataract surgery (RLLR) are very much up to the task of tackling these cataracts. In fact, these cataracts are usually softer than regular nuclear cataracts and are easier relatively to remove.
What are Senile Cataracts?
These are cataracts which occur due to degenerative changes in the lens in old age. In India it usually occurs after the age of 40 years. By the age of 70 years in India, more than 50% per cent of the normal population have, or have had, cataracts. It usually affects both eyes, but often develops in one eye earlier than in the other.
Senile cataracts have a strong genetic tendency and may appear earlier with each succeeding generation.
What are the symptoms of a Cataract, basically what should the patient look for?
The most frequent symptoms of a cataract are
- Diminished vision and glare -In the early stages only distance vision may suffer or the oncoming headlights at night can cause unbearable glare. Glare is caused by light rays unevenly entering the eye as cataract starts to form. Glare is frequently the very first symptom of cataract. In today’s day and age inability to see oncoming traffic due to their powerful headlights causing glare can prove fatal
- As a cataract progresses reading vision can suffer along with a change in spectacle number. People who were forced to wear reading glasses earlier will find that they can go without them. This is called second sight and indicates the formation of a cataract
- Sometimes because of swelling of the cataract, the pressure in the eye goes up and the patient complains of mild heaviness or headache
- Many a time the person will just say,”Dr nowadays when I read for an hour or two I get a heaviness of the forehead despite wearing the correct reading glasses”. This is because the human lens has become “dysfunctional and is causing the muscles in the eye to strain with near point activity. Today early cataract is called “Dysfunctional lens syndrome”. Luckily Catalys RLLR is a quick and easy solution
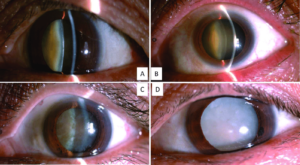
What is the early (incipient) stage of Cataract and what are its symptoms?
The patient can still read the last line of the vision chart. There is a mild blurring of vision in the eye developing a cataract. Distant objects seem to be slightly hazy, like looking through 8 am morning smog on Marine drive!. The patient may have to change the spectacle number but the vision is still a bit blurred. This called a dysfunctional human lens. Nowadays we do RLLR and change the lens. The person gets the benefit of a clearer vision and is spectacle free in most cases.
What is the immature stage of Cortical Cataract and its symptoms?
This is the next stage of cataract and is characterized by a noticeable decrease in vision, easily measurable on a vision wall chart. Despite the best spectacle correction, the vision progressively reduces. The fall in vision is for both distance and near. The patient will remark that they cannot read the bus number and signboards. Please remove the cataract asap.
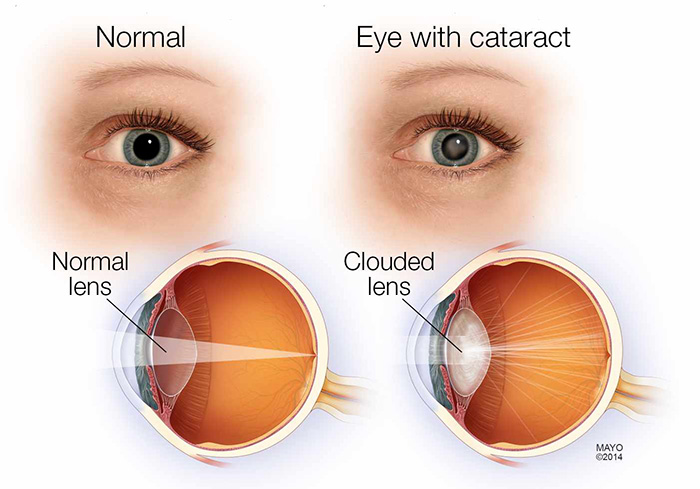
What is a Mature Cataract?
- The patient with a mature cataract will have a white opacity right in the middle of the eye. This white spot is the mature cataract visible in the open pupil.
- Vision is very very poor. The patient can, however, still see his fingers and can count them.
- Surgery should really be done at a much earlier stage as leaving the cataract in for too long, may result in irreversible damage to the eye. Remember as with most diseases “EARLIER the treatment the BETTER is the result.”
- A mature cataract is a swollen lens. A swollen lens pushes the iris forwards. This may narrow the outflow angle of the eye leading to increased eye pressure. So, remove a mature cataract as soon as it is detected.
What is Hypermature Cataract? What are the problems of Hypermaturity?
- A cataract, if left undisturbed after achieving maturity, tends to pass on to the hypermature stage.
- This stage is nowadays rarely seen, for it is essentially a result of neglect on the part of the patient or their relatives.
- In this stage, the lens tends to shrink and contents shrivel up. If the lens stays in its place, it tends to develop calcified spots, the capsule thins, the fluid of the lens occasionally leaks out leading to severe pain and inflammation, following which the eye is usually lost, unless attended to as an emergency.
- A Hypermature lens must be removed, as more often than not, it will lead to a rise in eye pressure which will be uncontrollable by medical means.
- In these cases, both mature and hypermature the support system of the lens is damaged as well and becomes “loose” like a loose elastic on your pyjama. When we fix these cases we frequently need to implant a device called a “tension ring” which gives the capsular bag where we are implanting the lens proper stability.
Any pain and redness in a cataract eye mean visit the doctor SOON!
Phacoemulsification (Ultrasound Cataract Surgery)
Till 2007 the most exciting innovation in cataract surgery, of this century was the technique of phacoemulsification. A New York ophthalmologist, Charles Kelman developed the technique in 1967, but it took over 20 years for the technique and the instrumentation to reach the level of sophistication, to make this a safe and acceptable form of cataract surgery.
In India the pioneer for this surgery was the authors father Padmashri Dr Keiki Mehta way back in 1987.
Why is Phacoemulsification sometimes called “Needle Surgery”?
Phacoemulsification (Phakos (greek) = Lens; Emulsify = to disperse finely) In phacoemulsification only a small needle penetrates into the eye through a very small opening. Using the latest sutureless method, the needle is inserted via a small tunnel, which is self-sealing. Thus at the end of the surgery even the needle track closes behind leaving, in time, no trace of its entry.
Why is Phacoemulsification mistakenly called Laser Beam Surgery?
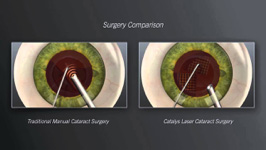
Actually in cataract surgery, only one true laser is used and that is the Robotic Femto laser in the procedure called Catalys Femto (RLLR)
Phaco is NOT laser cataract surgery
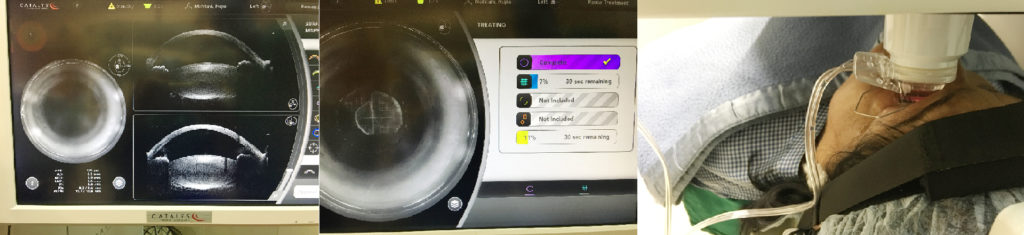
Why is Catalys RLLR called Instant Cataract Surgery?
Since the tiny laser cut opening heals rapidly, and the patient recuperates almost “instantly”. Hence this technique is termed “Instant Cataract Surgery”.
Is Phaco as good as RLLR (Robotic Surgery)
Not at all. Till we got a laser system in 2014 we never realised its benefits. Now once we have done thousands of cases on the laser system the benefits are evident. The eye heals faster and the lens is precisely centered. I still perform Phaco routinely as RLLR is not necessary for every case and it adds to the cost of surgery.
So which is the best Phaco System in the market?
Today the Centurion Active Sentry is the best system in the world but is very expensive. The average Phaco System is 12-15 lacs.
Centurion platforms are over 50 lacs. We have 2 of them and have been using them for 4 years now.

What is OziL and Active Sentry ?
Ozil is oscillatory or torsional phaco and is part of the Centurion system. Here the tip moves not forward and back but sides to side at 29,000 Hz. Here it generates much less heat than regular phaco and is very useful in the so-called “Cold Phaco”. Ozil is most useful in very hard cataracts.
Active sentry is a 2020 invention where the eye pressure is precisely maintained during surgery so that it recovers much faster and the surgery is much smoother. We have the first one in the country.
What is the immediate post operative care following Robotic Laser Lens Replacement (RLLR) Cataract Surgery ?
- On the day of surgery, one can sit up immediately move around, and walk around freely, sit in a chair, chat with his relatives and friends, etc. You can use your iPad, phone and conduct your normal business.
- You cannot put water in the eye for 10 days.
- The patient is free to use a pillow and can sleep on both sides on day 1 after surgery provided a small protective shield is securely taped into place.
- There are no restrictions on the diet of any kind.
- If the patient does not feel sleepy at night, it is perfectly acceptable to take a sleeping tablet.
- The patient continues all the medicines he routinely used to take for his other ailments, like blood pressure, diabetes, arthritis, etc.
- You can go for a walk the next day with your protective spectacles.
- After 3-4 days you can go back to the gym or perform yoga but no headstands, please.
Why does a RLLR procedure cost more than a routine Cataract Surgery ?
A computerised Cataract removal laser system like the CATALYS is an extremely costly piece of equipment (3 crores ), with a costly service warranty. It needs expert servicing at regular intervals sometimes weekly. The active sentry centurion is upwards of 50 lacs. There are not more than a dozen institutes in the whole country with this combined Cataract suite.
In, addition, one has to use a high powered microscope(UPTO 3 crores) which permits great depth of field coupled with extremely sharp optics coupled to zoom magnification.
Nowadays we use a digital microscope and operate by looking through 3D glasses on a screen.
Also to comply with American European regulations these new machines use disposable cassettes and tubes, which are very sensitive to pressure changes and need to be replaced for every case which costs a lot.
However, the great safety, security, speed, sterility and stability offered by these advanced machines procedure make the cost well worthwhile. The rapid rehabilitation means one can return to ones job earlier. The advantage thus far outweighs the extra cost of the procedure.
If these modern machines are so good then why doesn't everyone use them?
The basic cost of instrument is high.
Training is expensive some of it in foreign countries.
Maintenance cost of machines are high.
Given time, in about 10 years from now, every surgeon will be doing a cataract with a laser even in villages – it is inevitable, as the results will automatically dictate its usage.
In the cities its like the chicken and the egg story. If there aren’t enough patients to pay a reasonable amount, the doctor cannot afford to buy new machines and if the doctor does not have new machinery results may suffer and he does not get that many patients to buy expensive machinery.
Which Lens shall I have implanted in my eye?
In the olden days all lenses were made of a hard non foldable plastic and the eye was cut open 7 mm to let them in
Nowadays most lenses are “injectable” and enter the eye through a 2 mm opening called a tunnel which seals without any sutures.
Barring that the type of lens depends on whether
- You are going to read a lot-EDOF lens is best
- Lawyer ,Architect,Engineer or doctor-EDOF lens is best
- Lot of night driving-Use a tinted yellow lens for less glare not a multifocal. If you want spectacle independence use a EDOF lens
- Cost and affordability-Good lenses range between Rs 10,000-1 lac
- Whether you have diabetes or uveitis-material should be Soft Acrylic and not Silicone
Many other factors the doctor in his or her experience will decide.

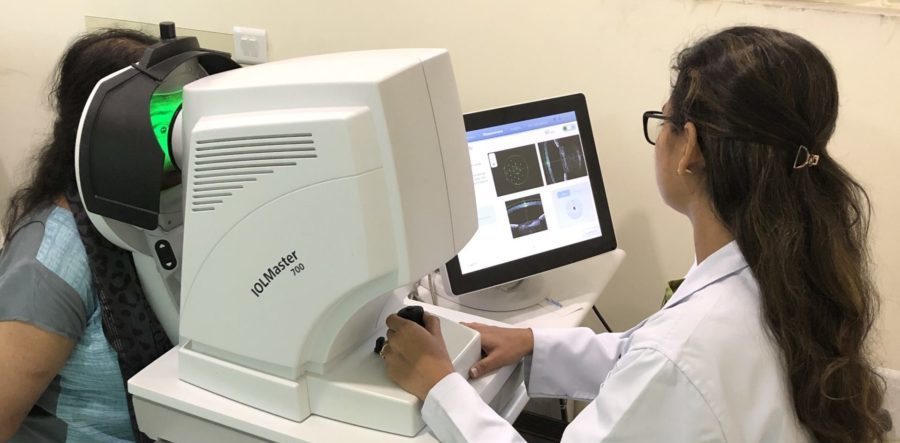
How is the power of an Intraocular Lens Calculated?
Computerised axial biometer-The A scan
A beam of ultrasound is aimed into the eye by touching a probe to the eye. It bounces back from the back of the eye. A computer calculates how long it took to return and knowing the speed of sound in the eye determines the length of the eyeball.
These measurements combined with a measurement of the curvature of the eyeball. These measurements go into complicated formulae for the final result! All this takes about 10-20 seconds.
The latest version is the IOL Master 700 TK from Zeiss Germany which we have been using for 3 years. It takes more than 60,000 measurements using a swept-source OCT. Basically like in the ironman movies it uses a laser scanner to create a 3D model of the eye and can calculate what size and power of the lens to implant so that you are left with just + or – 0.5.
Why doesn’t everyone use an IOL Master 700 TK
Once again cost. The average system to measure lens power is 2 lacs. This new device is 35 lacs and needs a specially trained technician.
Before the year 2000, all lenses implanted in the eye were Mono focal. Every patient got spectacles both for near as well as in most cases for far.
In 2000-2001 multifocal lenses were invented and we started implanting them. These were “bifocal implants” so the person could see far and near at 12-14 inches. Naturally for computer distance ie 18-22 inches they still needed a small spectacle number. In 2012 TRIFOCAL multifocal implants were invented by Zeiss in Germany. Today all multifocal lenses are Trifocal.
The problem with Bifocal or Trifocal Implants were that there was some amount of glare at night. This was variable, some patients would have a lot of glare and see haloes around lights at night to the extent that night driving became difficult. Some patients never had any glare at all. Even so in a few months the glare reduced to acceptable levels.
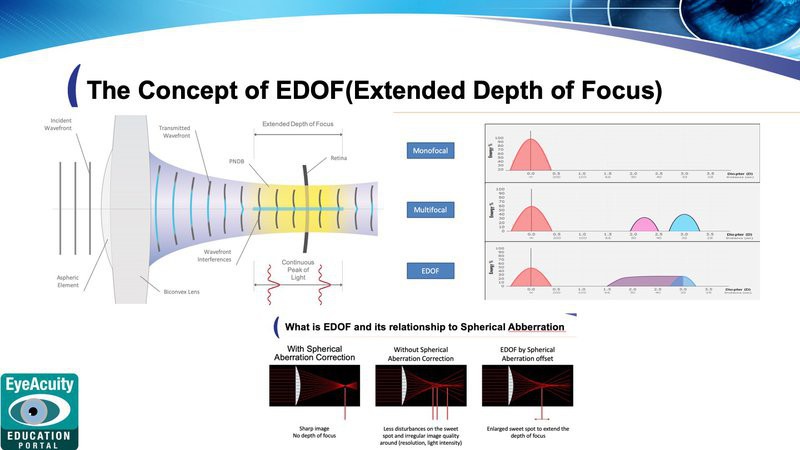
With the popularity of reading and searching social media and emails on the phone and iPads supplanted conventional books and printed material more and more people wanted good intermediate vision to eliminate the problem of glare and still give good intermediate vision and somewhat acceptable near vision EDOF(Extended Depth of Focus ) lenses were invented. With these new implants, people could see distance well with no glare or haloes at night and could read and use their devices. Sometimes with these EDOF lenses, the person may still need a small reading number. The advantage is no glare and spectacle independence most of the time.
EDOF lenses are the latest lens tech in 2020.
To implant, an EDOF or even an older trifocal lens perfectly an RLLR Laser System does a better job than conventional Phaco surgery as the lens placement is more precise. Even decentering these lenses by 1mm leads to bad vision. Only an opening made to micron perfection by a true laser system can give us this precision.
The Concept of EDOF
How do these Multifocal Lens work? How do they differ from Bifocal Spectacle Glasses?
These TRIFOCAL lenses work by creating three focal points. One for distance, and the second for intermediate ie computer or phone distance at 20 inches and the third focal point at 12 inches for near. Thus one can see for both distance and near. However a very important difference between multifocal implants and bifocal spectacles is that, the spectacle has a single focus at any one time, i.e. one can either see only distance (from the upper segment) or only near (from the lower D segment). While with a multifocal implant, all images are being formed simultaneously, all the time.

How does the patient benefit from a Multifocal / EDOFimplant ?
It provides for both distance and near and to some extent even intermediate range. Thus there is greater range of depth for focus available as compared to a Unifocal (i.e. a single focal) implant.
Another important advantage is the clarity for medium distance images i.e. in the intermediate range. A patient fitted with a EDOF Implant is better able to adjust himself in the normal daily activities and can cook food, do house work even play golf, and billiards and cards with ease. It thus makes for a more comfortable natural vision.
When a patient has a Multifocal Implant, does that mean he will wear no glasses for distance at all ?
Even with an implantation of a multifocal implant, some spectacle MAY be needed for distance and, May be some for near. However the power is usually quite small. Despite the best of care, with the latest computerised instruments, and using some of the finest technology in the world, some spectacle number for distance will always be present. The University of Miami, USA, in an analysis of their cases concluded that only 14% of their eyes reach a zero power following surgery, while 86% will have some residual power.
The important factor about Multifocal/EDOF implants is Not that one can do totally without glasses, (which is sometimes impossible), but that one would not be dependant on glasses.
Does the presence of a Multifocal / EDOFimplant mean that no reading glass will be required ?
Under normal circumstances, no reading glasses are needed over the distance requirements. However this statement holds true only for reasonable sized print, typewritten or medium sized newsprint, and provided adequately well focussed light is available. If very fine letters are to be seen (e.g. classified advertisement in the news paper or the labels on drug bottles and ampoules, then small additional reading spectacle is required. Ideally good light at a distance of 3-4 feet from the reading material is the best.
It would be reasonable to say that once fitted with multifocal/EDOF implant for almost 90% of ones daily activity, reading spectacles may not be needed.
Who makes these EDOF Lenses ?
Companies from USA Switzerland Germany and Italy have all got good EDOF lenses on the market.
Why does a patient choose a EDOF over an Unifocal Lens in the first place ?
The basic reason for a EDOF is simple. The patient would like to do away with dependence on glasses. It is likely that for 90% of a patient’s daily working life additional spectacle correction for near may not be needed. To many patients, this unobstructed vision is important. To an executive dealing with an important client, a salesman making to final pitch, a businessman negotiating the closing of a deal, all require an unimpeded vision. The distraction of a pair of reading spectacles is just not acceptable.
The Multifocal also enhance intermediate range of vision sporting activities like playing golf, badminton and tennis or even carrom and table tennis become infinitely easier.
The freedom to go to a restaurant or a party ,or see the mobile phone and to read without having to reach for the reading spectacles makes it, for many, an excellent proposition.